SAA – Systematic Qualitative Review of Computerized Interventions for Adolescents: Implementation in Emergency Departments and Trauma Centers
SAA – Systematic Qualitative Review of Computerized Interventions for Adolescents: Implementation in Emergency Departments and Trauma Centers
 SAA – Systematic Qualitative Review of Computerized Interventions for Adolescents: Implementation in Emergency Departments and Trauma Centers
SAA – Systematic Qualitative Review of Computerized Interventions for Adolescents: Implementation in Emergency Departments and Trauma CentersA submission by Students Against Addiction Systematic Qualitative Review of Computerized Interventions for Adolescents: Implementation in Emergency Departments and Trauma Centers
[space value=”20″]
[divider icon=”adjust” style=”none”]
Abstract
Objective: To evaluate the effectiveness of Computerized Alcohol Interventions for the adolescent population. A qualitative systematic review of randomized controlled trials was carried out to investigate the current state of research.
Methods: Three main databases (PUBmed, Medline, and Web of Science) were searched for relevant randomized controlled trials (RCT) that measured the effects of computerized alcohol interventions on the adolescent population (<18 years of age). Other reviews on the subject were checked for missed RCTs. Characteristics of the studies were summarized and abstracted.
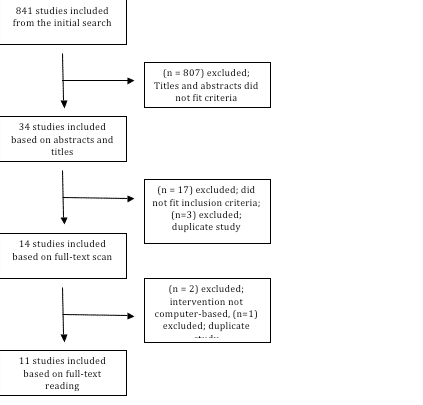
Results: Using the initial keywords, 841 studies were discovered to be relevant to the topic. Of those trials, only 11 fit the inclusion criteria of the review.
Conclusion: Overall, the majority of included studies concluded that computerized brief interventions (BI) are effective in altering drinking behavior in the adolescent population; however, there is a lack of RCTs on the topic. Thus, further research is required before a definitive conclusion is made on the effectiveness of implementing computerized interventions for adolescents in the emergency departments or hospital setting is appropriate.
Keywords: alcohol, intervention, computer, adolescent, CASI, emergency department, trauma centers.
INTRODUCTION
Adolescents are at risk of developing hazardous drinking behavior because experimentation is prevalent in these formative years1. Surveys indicate that there is an increasing trend in alcohol consumption from 8th to 12th grade with 12% and 29% of students drinking five or more drinks in the past two weeks respectively2. Cognitive abilities may be impaired due to constant alcohol consumption3, 4.
Alcohol use in the United States has been associated to injury and harm5. It is a significant contributor for adolescent fatalities such as motor-vehicle crashes, homicide, and suicide6. Alcohol is also a primary reason for high-risk sexual encounters and sexual assault6. Adolescent drinking patterns are dangerous because they have a higher incidence of binge drinking7. In the 2005 National Youth Behavior Risk Survey, 26% high school students nationwide admitted to have had at least one binge drinking (more than five drinks in a row in one occasion) episode on the past 30 days. Additionally, 29% of high school students nationwide had ridden in vehicles that were driven by someone who has been drinking and 10% of high school students nationwide had driven after drinking8.
Most of the injured and non-injured adolescent alcohol drinkers end up in emergency departments (ED) and in trauma centers9-11. Implementation of screening and interventions in these settings might prove useful12. However, there is limited information about interventions targeted to adolescents13. Trauma centers and EDs may provide unique opportunities for teachable moments with at-risk adolescents14. Novel modalities, such computers and the internet, may provide an opportunity for healthcare providers to deliver interventions to the younger population in a rapid and efficient manner.
The objective of this qualitative systematic review is to compare the different computerized interventions aimed at reducing alcohol consumption in the adolescent population. The review will capture the current state of the research and identify any gaps or weaknesses in the included randomized controlled trials (RCT). Other systematic reviews have investigated the effects of computerized interventions in the adult population but few studies have specifically probed the value of it in the adolescent population15-18. Computerized intervention is a new frontier that is yet to be explored and its benefits include cost-savings, convenience, accessibility, and anonymity.
METHODS
Search Strategy
The following databases were searched with no restriction on date of publication: Pubmed, Medline, and Web of Science. The keywords used include alcohol, brief intervention, computerized, computer, screening, adolescence, and adolescent. MeSH terms were included for a more thorough search. Additionally, references of systematic reviews on computerized alcohol interventions were scanned for possible inclusion. Unpublished data was acquired through conference proceedings through Web of Science. Only studies in English were included in the review. Search terms used were determined by reviewing related articles and thorough discussions with a librarian information specialist.
Selection Criteria
Only studies with randomized controlled trials were included. Population was limited to adolescents (12 – 17 years old). The intervention must aim to alter one’s behavior using the computer as the main vehicle of delivery (online, offline, kiosk, CD-ROM, etc.). All studies that used a computer (even with supplemental support) were included in the review. Studies that compared computer interventions with either an active or minimally-active comparator group were included in the review.
Study Screening
References identified through the search were initially screened by reading their title and abstract. Any study related to alcohol interventions for adolescents was included through the next step of screening. Special attention was given to the method of delivery of the intervention and the mean age (>18 years old) of participants. The references of the included studies were also reviewed to determine the relevance for inclusion. The final screened studies were read in full text and critical components have been summarized in the tables below (Table 1-4)
Results
Study Description
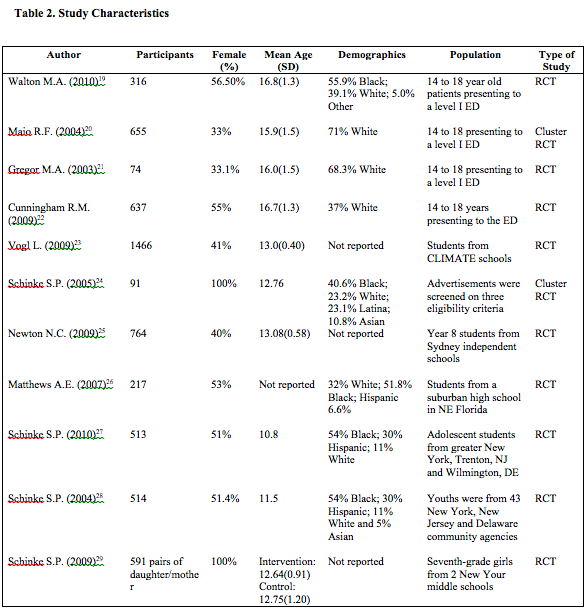
The search yielded 11 studies for inclusion into this scoping review19-29 (Table 1). The most dated study was published in 2003 while most studies were published recently in 2009 and 2010. Computerized intervention for teenagers is still in its infancy and therefore only a few studies in the field have been published. During the search, broader search terms were used until the final terms listed above yielded sufficient studies for a scoping review. The setting was not limited to emergency departments and trauma centers because the advantage of computerized interventions is its uniform delivery of content and its accessibility; therefore, place of intervention should not be a factor in the result.
Study Characteristics.
Students in middle school were studied by four of the included trials (n=4)23, 29, 25, 26. Another four studies concentrated on adolescents presenting in emergency departments or trauma centers (n=4)19, 20-22.The majority of studies did not implement any screening instrument for alcohol consumption and allowed all volunteers to participate as long as they consented (n=9) 20, 21, 23-29. Only one study used a validated screening instrument, the Alcohol Use Disorders Identification Test (AUDIT), to screen for alcohol use disorder (AUD)22. Another study used a survey that asks for alcohol consumption in past year19.
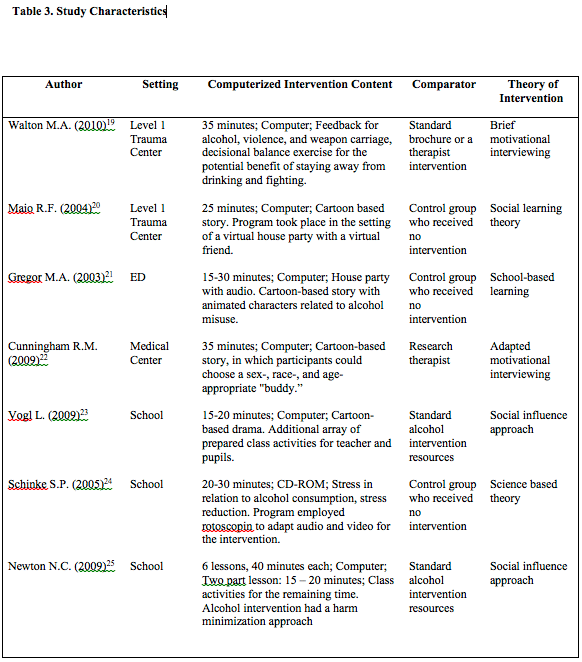
Comparator groups differed in each trial. Most studies compared the computerized intervention group against a control group who received no intervention (n=5)20, 21, 24, 27, 28. Four trials compared the computerized intervention group against a control group receiving “standard” interventional resources (n=4)19, 23, 25, 29. Only two studies compared the computerized intervention group to a live research therapist (n=2)19, 22. Only one trial compared an interactive computerized intervention against a non-interactive computerized intervention26 (Table 3).
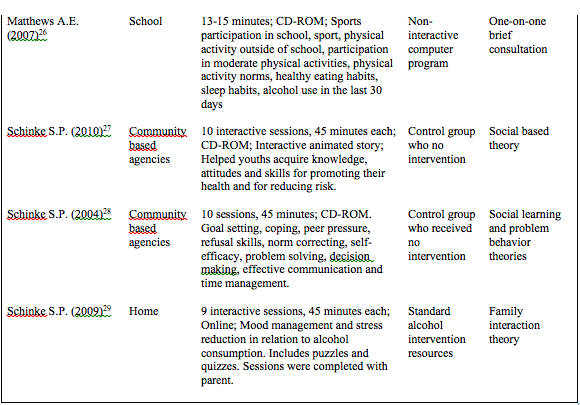
The majority of the computerized interventions were delivered in a setting determined by the researcher, such as EDs or schools. Four studies implemented the intervention at the teenagers’ school (n=4)23-26. Other locations were emergency departments and trauma centers (n=4)19-22 Two studies used community-based agencies to carry out the intervention (n=2)27, 28. Only one study allowed the participants to complete the intervention through a private home computer29.
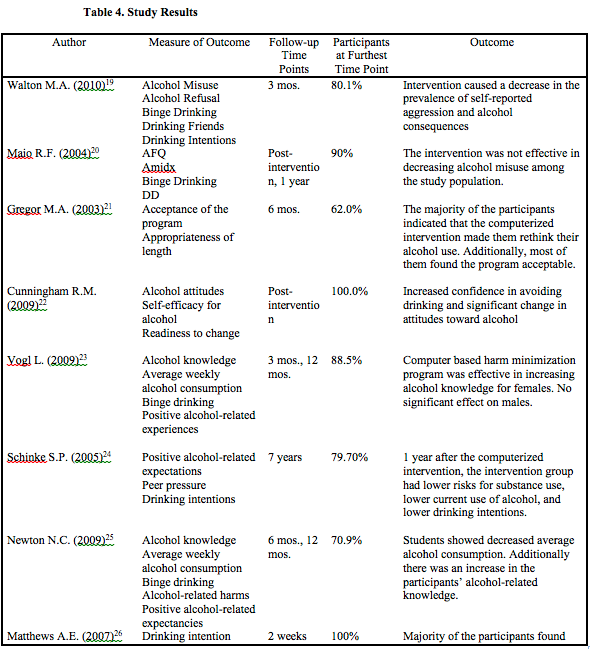
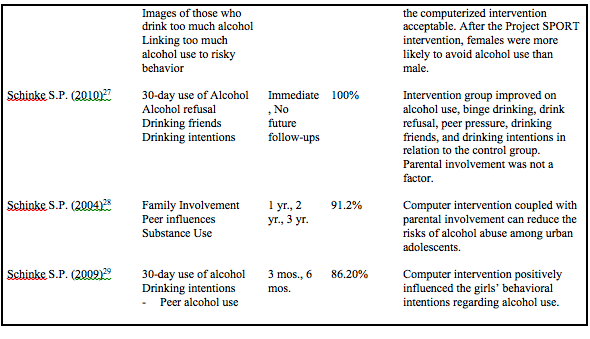
The types and contents of each intervention from the included studies vary greatly. Most interventions consist of an engaging virtual environment or interactive cartoon story where an adolescent can explore the consequences of drinking alcohol accompanied by a digital “buddy” (n=5) 20-22, 23, 27. The “buddy” acts as an older, wiser friend who gives advice about proper drinking. One intervention includes puzzles and quizzes to reinforce the content of the intervention and to keep an adolescent’s attention to the program29. Another study uses a computerized intervention in conjunction with classroom activities23, while two studies included a family member to aid in the intervention28, 29. Finally, there are studies that have traditional questions in text and recommendations for changing one’s drinking behavior (n=2)19, 26 (Table 4).
The most common measure of outcome among the eleven studies is the participant’s ‘intention to consume alcohol’ (n=5)19, 24, 26, 27, 29. Another common measure between the studies is ‘binge drinking behavior’ (n=4)19, 20, 23, 25. ‘Peer induced drinking behaviors is the third most prevalent measure (n=3)29, 24, 28 followed by ‘knowledge about alcohol’ (n=2)23, 25. In the 11 studies included in the review, there is no common measure of outcome that was implemented by all the trials; therefore, conducting a meta-analysis is not feasible.
Overall, the studies concluded that computerized brief interventions were effective in altering the participants’ drinking behavior or attitude towards alcohol consumption. Only one study asserted that the intervention had no effect27. The majority of the studies reported decreased intention of drinking for their participants (n=3)21, 27, 29. Another trend that was significant was the increase in alcohol knowledge among the adolescents (n=3)23, 25, 26. Average alcohol consumption was reported to have decreased in three study populations (n=3)23-25. Other studies indicated a general positive change in other risk factors for alcohol abuse. A few studies commented on the disparity in response between boys and girls (n=2)23, 26.
DISCUSSION
Generally, treatment for adolescent alcohol use is limited. According to the
National Institute of Alcohol Abuse and Alcoholism (NIAAA), there are 1.4 million youth that meet the criteria for alcohol abuse or dependence; however, only 227,000 receive some form of treatment. The institute released the following recommendations for creating a treatment of alcohol use disorder tailored to the specific needs of adolescents: (1) Easy access to treatment and geared toward their age group; (2) Adolescent’s perception that traditional methods (e.g. alcoholic treatment programs, Alcoholics Anonymous) are less helpful than brief interventions30. These criteria are met by computerized brief intervention modalities.
Screening for AUD have been developed, validated, and refined for adolescents and adults31-34.Studies indicate that computerized alcohol screening instruments are just as effective as identifying individuals with hazardous drinking behaviors compared to in-person interventions35. Additionally, Weisband et al concluded that computer forms may increase self-disclosure from the user36. Interventions modalities following an alcohol screening are diverse and they have been used in trauma centers and emergency department37. Tait et al showed that emergency department-based interventions encouraged 32% of adolescents to attend an AUD treatment agency compared to 4% of adolescents who received the usual care38. From this scoping review, all but one of the included studies concluded that computerized interventions may reduce adolescent alcohol drinking and consumption. Moreover, the strong correlation of adolescent harm and injury with alcohol indicates that some form of additional treatment may be necessary. Therefore, computerized interventions may be suitable for inclusion into an adolescent patient’s standard of care in the ED or trauma center.
To fully appreciate the true effects of computerized alcohol interventions for the adolescent population, a few challenges and limitations must be overcome. First, there is a lack of randomized controlled trials testing the effectiveness of the computerized intervention. The initial search for trials for inclusion into this review yielded only a small number of studies. All but one of the included studies concluded that computerized interventions may reduce alcohol drinking and consumption; however, each study has their own measure of outcome making it difficult to gauge its true effects. Although the effects of these interventions show promising results, continued research on the topic can confirm the results.
Second, a standard measure should be implemented to streamline the comparison between different trials. It was difficult to assess which interventional content, length, or setting was best because of the differing measures of outcome. The best measure of outcome for an adolescent participant may be the number of binge drinking episodes because of the population’s unique drinking pattern. As mentioned earlier in the review, adolescents are more likely to partake in less drinking sessions, however, they drink more in those sessions. Another measure that might be helpful is the amount of alcohol consumed by an adolescent in a given time period. A measure of consumed alcohol in grams or ounces would establish a concrete measure of intervention impact that would be free from self-reported bias.
Finally, it must be determined if the setting of the intervention has any bearing on its effectiveness. All the included trials conducted their intervention in only one place. An interesting trial might compare the result of an intervention done in different settings such as a school or an ED. Studies can also focus on specific settings such as the ED or trauma center.
Conclusion
The dangerous drinking habits of the adolescent population, hazardous psychosocial behaviors associated with drinking, and the concomitant risk for injury and death make the computerized intervention program a feasible deterrent in the ED or trauma center. A meta-analysis should be done to confirm the effectiveness of these alcohol adolescent interventions with the limited setting of only the ED or trauma center. The overall positive impact and adolescent acceptability of computerized intervention make it an ideal candidate for effectively preventing alcohol misuse in the adolescent population. A few minutes interacting with a computer could prevent a lifetime of regrets and disappointments.
The Best Call You Will Ever Make
Call Now to Speak Confidentially with an admission counselor.
References
- Thatcher DL, Clark D. Adolescent Alcohol Abuse and Dependence: Development, Diagnosis, Treatment and Outcomes. Curr. Psy. Rev. 2002; 2(1): 159-177
- Faden VB, Fay MP. Trends in Drinking Among Americans Age 18 and Younger: 1975-2002. Alcoholism: Clin. And Exp. Research. 2004; 28(9): 1388-1395
- Chambers RA, Taylor JR, Potenza MN. Developmental Neurocircuitry of Motivation in Adolescence: A Critical Period of Addiction Vulnerability. Am. J. Psy. 2003; 160(6): 1041-1052
- Brown SA, Tapert SF; Adolescence and the Trajectory of Alcohol Use: Basic to Clinical Studies. Ann. N.Y. Acad. Sci. 2004; 1021(1): 234-244
- Sindelar HA, Barnett NP, Spirito A. Adolescent Alcohol Use and Injury: A summary and critical review of the literature. Minerva Pediatr. 2004; 56(3): 291-309
- National Institute on Alcohol Abuse and Alcoholism. Underage drinking: a major health challenge. Alcohol Alert. 2003; 59
- Clark DB, Bukstein OG. Psychopathology in Adolescent Alcohol Abuse and Dependence. Alc. Health Res. World. 1998; 22(2): 117-121
- Eaton DK, Kann L, Kinchen S et al. Youth Risk Behavior Surveillance—United States. J. Sch. Health. 2005; 76(7): 353-372
- Bates BA, Shannon MW, Woolf AD. Ethanol-related Visits by Adolescents to a Pediatric Emergency Department. 1995; 2(2): 89-92
- Maio RF, Portnoy J, Blow FC, Hill EM. Injury Type, Injury Severity, and Repeat Outcomes of Alcohol-Related Trauma in Adolescents. Alcohol Clin. Exp. Res. 1994; 18(2): 261-264
- Mannenbach MS, Hargarten SW, Phelan MB. Alcohol Use among Injured Patients Aged 12 to 18 years. Acad. Emerg. Med. 1997; 4(1): 40-44
- Chung T, Colby SM, Barnett NP et al. Alcohol Use Disorders Identification Test: Factor Structure in an Adolescent Emergency Department Sample. Alcohol Clin. Exp. Res. 2002; 26(2): 223-231
- Newton AS, Gokiert R, Mabood N et al. Instrument to Detect Alcohol and Other Drug Misuse in the Emergency Department: a systematic review. Pediatrics. 2011; 128(1): 180-192
- Delgado KM, Ginde AA, Pallin DJ et al. Multicenter Study of Preference for Health Education in the Emergency Department Population. Acad. Emerg. Med. 2010; 17(6): 652-658
- Rooke S, Thorsteinsson E, Karpin A, et al. Computer-delivered Interventions for Alcohol and Tobacco Use: a meta-analysis. Addiction. 2010; 105(8): 1381-1390
- Khadjesari Z, Murray E, Hewitt C, Hartley S et al. Can Stand-Alone Computer-Based Interventions Reduce Alcohol Consumption? A systematic review. Addiction. 2011; 106(2): 267-282
- Carey KB, Scott-Sheldon LA, Elliott JC et al. Computer-Delivered Interventions to Reduce College Student Drinking: a meta-analysis. Addiction. 2009; 104(11): 1807-1819
- Bewick BM, Trusler K, Barkham M et al. The Effectiveness of Web-Based Interventions Designed to Decrease Alcohol Consumption—a systematic review. Prev. Med. 2008; 47(1): 17-26
- Walton MA, Chermack ST, Shopet JT et al. Effects of a Brief Intervention for Reducing Violence and Alcohol Misuse among Adolescents. JAMA. 2010. 304(5): 527-535
- Vogl L, Teesson M, Andrews G et al. A computerized harm minimization prevention program for alcohol misuse and related harms: randomized controlled trial. Addiction. 2009; 104(4): 564-575
- Schinke SP, Schwinn TM, Fang. Longitudinal Outcomes of an Alcohol Abuse Prevention Program for Urban Adolescent. J. Of Adolesc. Health. 2010; 46(5): 451-457
- Schinke SP, Fang L, Cole KC. Preventing substance use among adolescent girls: 1-year outcomes of a computerized, mother-daughter program. Addict. Behav. 2009; 34(14): 1060-1064
- Schinke SP, Schwinn T. Gender-Specific Computer-Based Intervention for Preventing Drug Abuse among Girls. Am. J. Drug Alcohol Abuse. 2005; 31(4) 609-616
- Schinke SP, Schwinn TM, Di Noia J et al. Reducing the Risks of Alcohol Use among Urban Youth: Three-year Effects of a Computer-based intervention with and without parent involvement. J. Stud. Alcohol. 2004; 65(4): 443-449
- Newton NC, Vogl LE, Teesson M et al. CLIMATE Schools: alcohol module: cross-validation of a school-based prevention program for alcohol misuse. Aust. N. Z. J. Psychiatry. 2009; 43(3): 201-207
- Matthews AE, Werch C, Michniewicz M et al. An Impact Evaluation of Two Versions of a Brief Intervention Targeting Alcohol Use and Physical Activity among Adolescents. J. Drug Edu. 2007; 37(4): 401-416
- Maio RF, Shope JT, Blow FC et al. A Randomized Controlled Trial of an Emergency Department-Based Interactive Computer Program to Prevent Alcohol Misuse among Injured Adolescent. Ann. Of Em. Med. 2004; 45(4): 420-429
- Gregor MA, Shope JT, Blow FC et al. Feasibility of Using an Interactive Laptop Program in the Emergency Department to Prevent Alcohol Misuse among Adolescents. Ann. Of Em. Med. 2003; 2, 276-284
- Cunningham RM, Walton MA, Goldstein A et al. Three-month Follow-up of Brief Computerized and Therapist Interventions for Alcohol and Violence among Teens. Acad. Emerg. Med. 2009; 16(11): 1193-1207
- National Institute on Alcohol Abuse and Alcoholism. Underage drinking: Why Do Adolescents Drink, What are the Risks, and How can Underage Drinking be Prevented. Alcohol Alert. 2006; 67
- Clark DB, Moss HB. Providing Alcohol-Related Screening and Brief Interventions to Adolescents Through Health Care Systems: Obstacles and Solutions. PLoS Med. 2010; 7(3): e1000214
- Knight JR, Sherritt L, Harris SK et al. Validity of Brief Alcohol Screening Tests among Adolescents: a comparison of the AUDIT, POSIT, CAGE and CRAFFT. Alcohol Clin. Exp. Res. 2003; 27(1): 67-73
- Sindelar-Manning H, Lewander W, Chin T et al. Emergency Department Detection of Adolescent with a History of Alcohol Abuse and Alcohol Problems. Pediatr. Emerg. Care. 2008; 24(7): 457-461
- Levy S, Sherritt L, Harris SK et al. Test-retest Reliability of Adolescents’ Self-Report of Substance Use. Alcohol Clin. Exp. Res. 2004; 28(8): 1236-1241
- Chan-Pensley E. Alcohol-Use Disorders Identification Test: a comparison between paper and pencil and computerized versions. Alcohol Alcohol. 1999; 34(6): 882-885
- Weisband SP. Group Discussion and First Advocacy Effects in Computer-Mediated and Face-to-face Decision Making Groups. Organizational Behav. Human Decision Processes. 1992 53(3); 352-380
- Burke PJ, O’Sullivan J, Vaughan BL. Adolescent Substance Use: Brief Interventions by Emergency Care Providers. Pediatr. Emerg. Care. 2005; 21(11): 770-776
- Tait RJ, Hulse GK, Robertson SI et al. Emergency Department-based Intervention with Adolescent Substance Users: 12-month Outcomes. Drug Alcohol Depend. 2005; 79(3): 359-563